
Science has undergone a radical metamorphosis. People with M.D. or Ph.D. degrees, who have published hundreds of papers in the scientific literature, have suddenly become “anti-science”—as judged by media personalities, politicians, bureaucrats, and fact-checkers. What does this mean? One clue: chief White House medical advisor Anthony Fauci, M.D, said that anyone who attacked him was attacking “science.”
Anyone skeptical of the accepted COVID narrative may be called “anti-science.” The articles of faith are that it is an existential threat, and the only solution is universal vaccination and surrender of our freedom to work, assemble, worship, travel, or even go outdoors without the approval of public health authorities.
One key feature of science that we should’ve learned in grade school seems to have been forgotten, albeit selectively: experiments need to have a control group.

Ancient or medieval physicians may have said that bleeding and purging cured disease. The only time these cures didn’t work was when the patient was too far gone to be saved. The science was settled; no control group needed.
Doctors may like to imagine that we have godlike powers, but in fact we can never know what would’ve happened had we done something different.
That’s the reason why studies of treatment must have a control group. The “gold standard” is a double-blind randomized controlled study (RCT) to correct for observer bias and the placebo effect. Giving a fake medicine (placebo) sometimes helps.
Any experiment can have two types of error. Type I error “finds” a difference between the treatment and control group just because of random variation. A type II error fails to find a sufficiently large difference to reach “statistical significance” even though one exists. Studies need to be adequately “powered”—have an adequate number of subjects—to minimize type II error. A power of less than 80 percent is generally considered unacceptable. A study that is too small is called “underpowered.”
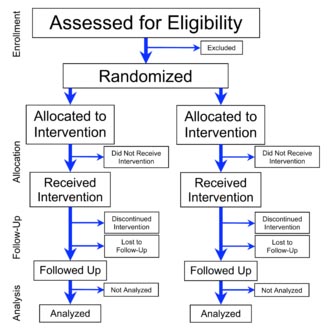
Ideally, there should be a 50:50 allocation of treated and control subjects. If only 30 percent of subjects are in the control group, the study loses significant power. If only 10 percent are in the control group, the power of the study is only 40 to 60 percent, writes Mark H. White, II, Ph.D. At the moment, about 30 percent of Americans have not taken the COVID vaccine. And government keeps trying to reduce that percentage to as close to zero as possible.
There was a 50:50 allocation in the preauthorization studies of the COVID vaccines. But the blinding has been broken, and those who received placebo are now eligible to receive active vaccine. Thus, there is virtually NO control group for potential late adverse consequences.
A large number of adverse effects are being reported to the Vaccine Adverse Events Reporting System (VAERS), including nearly 20,000 deaths as of Dec 10, vastly more than for all other vaccines combined. Reporting is far from complete. The actual number may be 20 to 41 times higher. As revealed by Project Veritas, reporting may be actively discouraged.
Did the vaccine cause these problems? We have no RCT that specifically looked for them, and a potential control group of only about 30 percent at present. The best we can do is look at “historical controls,” the reported past incidence of conditions such as myocarditis. Within 8 weeks of the public offering of COVID-19 products to 12-to-15 year-olds, the rate of myocarditis cases was 19 times the historically expected number.
Diseases vary over time for many reasons, and historical controls have many pitfalls. The historical natural history of the disease was nonetheless good enough for Anthony Fauci in his landmark 1973 research on Wegener’s granulomatosis in 18 (eighteen) patients.

Knowledge of the historical progression of AIDS was, however, NOT good enough for Dr. Fauci to inform physicians of the possibility of using common sulfa drugs to prevent pneumocystis pneumonia (PCP), based on past research. He demanded, but would not fund, an RCT. By the time a privately funded study was complete, 17,000 AIDS patients had died of PCP without the potential benefit of prophylaxis.
The NIH is again following the model of therapeutic nihilism for COVID, suppressing promising treatments on the basis that hundreds of favorable published studies including some RCTs are inadequate.
Vaccines, however, are exempt from the demand for scientific rigor. The Biden Administration is calling for all Americans to get vaccinated and boosted, and has pledged to donate 500 million doses of the Pfizer-BioNTech product to low and lower-middle-income countries and the African Union.
The worldwide, coercive mass vaccination campaign is not a scientific experiment. In addition to a control group, ethical research would require voluntary informed consent, free medical care of subjects who experienced complications, provision to stop the experiment if it is doing harm, and an Institutional Review Board.
Where is the science, and where is the anti-science?

About the author: Jane M. Orient, M.D. obtained her undergraduate degrees in chemistry and mathematics from the University of Arizona in Tucson, and her M.D. from Columbia University College of Physicians and Surgeons in 1974. She completed an internal medicine residency at Parkland Memorial Hospital and University of Arizona Affiliated Hospitals and was a lecturer at the University of Arizona College of Medicine and a staff physician at the Tucson Veterans Administration Hospital. She has been in solo private practice since 1981 and has served as Executive Director of the Association of American Physicians and Surgeons (AAPS) since 1989.
She is currently president of Doctors for Disaster Preparedness. She is the author of YOUR Doctor Is Not In: Healthy Skepticism about National Healthcare, and the second through fifth editions of Sapira’s Art and Science of Bedside Diagnosis published by Wolters Kluwer. She authored books for schoolchildren, Professor Klugimkopf’s Old-Fashioned English Grammar and Professor Klugimkopf’s Spelling Method, published by Robinson Books, and coauthored two novels published as Kindle books, Neomorts and Moonshine. More than 100 of her papers have been published in the scientific and popular literature on a variety of subjects including risk assessment, natural and technological hazards and nonhazards, and medical economics and ethics. She is the editor of AAPS News, the Doctors for Disaster Preparedness Newsletter, and Civil Defense Perspectives, and is the managing editor of the Journal of American Physicians and Surgeons.